Thyroid hormones play a very important role in healthy growth and development during childhood, impacting metabolism, the nervous system and organ functions.1 Therefore, it is vital that parents understand the signs and symptoms of thyroid disorders. It is also important to remember that treatments are available and that early intervention will help to avoid any long-term issues or complications.1
Children diagnosed with thyroid problems need the support of their families to ensure they take their medication regularly and understand their condition. It is also recommended that schools/nurseries are informed so that they are aware of the child’s diagnosis and medication requirements.
Meet Hypo and Hyper, the Thyroid Butterflies
In order to spot the symptoms associated with hypothyroidism and hyperthyroidism, think of them as butterflies, each with a different personality: Hypo (short for hypothyroidism) and Hyper (short for hyperthyroidism).
Meet Hypo, the slow and sluggish butterfly
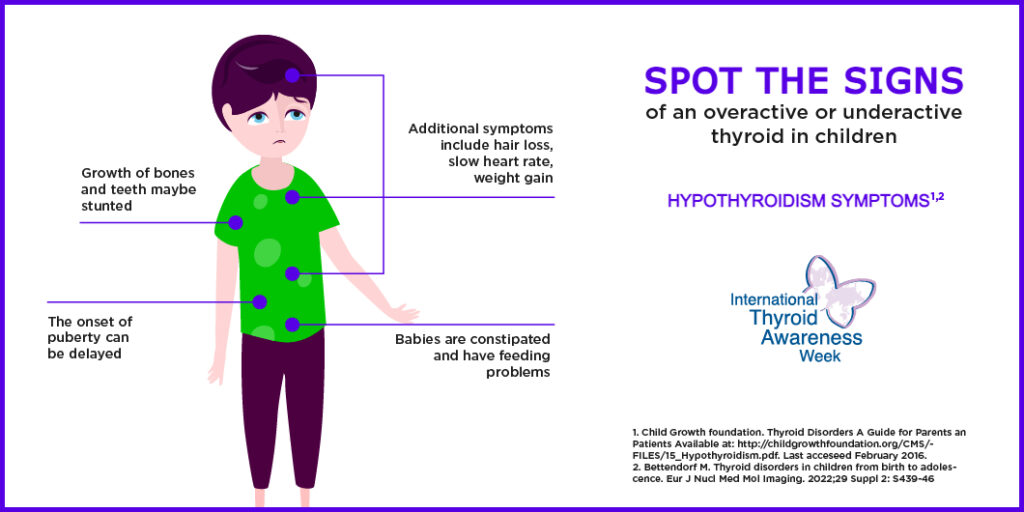
Hypo is a blue butterfly. He is slow moving compared with his friends and not growing as fast. He is often tired and sometimes sluggish. His skin is cold and his heart rate is slower than that of other butterflies.
Meet Hyper, the highly active and restless butterfly
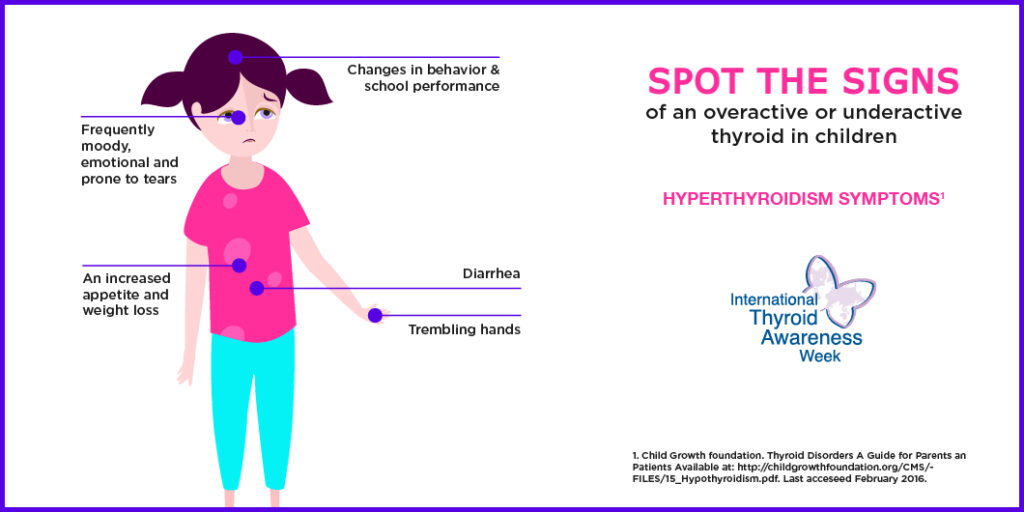
Hyper is a thin, overly active, fidgety pink butterfly. She is irritable and easily upset. She is often hungry and eats a lot, but is still losing weight.
Could my baby experience thyroid problems?
Children can experience thyroid problems from birth as they can be born without a properly working thyroid gland, a condition called congenital hypothyroidism.2 This condition can be difficult to spot at birth as babies may not have any symptoms, or may only display mild symptoms that often go unrecognized.2
What should I look for?
Typical symptoms of congenital hypothyroidism include:2
Prolonged jaundice
Excessive sleeping
Poor feeding
Poor muscle tone
Constipation
Cold extremities
To avoid the more serious effects of untreated congenital hypothyroidism – including impaired brain development – screening for every baby is recommended soon after birth. The preferred time for screening is typically a few days after the child has been born.2 Children with congenital hypothyroidism are treated with proper medication in the same way as adults.2 This treatment can ensure that the child continues to develop normally.2
If you are at all concerned that you or your child may be at risk for, or suffering from, thyroid problems, please discuss this with your doctor. To aid your consultation, download our Wellbeing Diary to help you keep a check of the symptoms you and/or your child is experiencing.
An underactive thyroid gland in children
The most common cause of acquired hypothyroidism in an autoimmune reaction.3 Hashimoto’s thyroiditis is a cause of acquired hypothyroidism where the body’s immune system attacks the thyroid gland and interferes with the production of thyroid hormones.4
The signs of hypothyroidism in children can vary depending on their age when the problem starts:
Babies may be jaundiced for longer than usual1
Older children may experience stunted growth in terms of their bones or teeth1
Children of school age may experience learning difficulties and puberty may be delayed1,3
Treatment
The goal of hypothyroidism treatment in children is to replace the missing thyroid hormone. The appropriate medication for hypothyroidism in adults are also recommended for use in children. However, the dose is tailored to match the specific weight and needs of the child.1
If you are at all concerned that you or your child may be at risk for, or suffering from, thyroid problems, please discuss this with your doctor. To aid your consultation, download our Wellbeing Diary to help you keep a check of the symptoms you and/or your child is experiencing.
An overactive thyroid gland in children
The autoimmune disorder Graves’ disease is responsible for almost all the cases of hyperthyroidism in children. Graves’ disease tends to be more common in teenagers than toddlers, and generally affects more girls than boys.1
Graves’ disease in children can often be difficult to identify because it develops slowly. However, there are common signs and symptoms to be aware of. These include:1
Changes in behavior and school performance
Sleeplessness or restlessness
Irritability
Needing to get up in the night to urinate
An enlarged thyroid gland
Trembling hands
Slight bulging of the eyes
An increased appetite but combined with weight loss
Fast heart rate
Nervousness
Diarrhea
Treatment
The goal of treatment in children with hyperthyroidism is to reduce the amount of thyroid hormone present in the bloodstream. There are several treatment options available, all of which are involved with possible complications and should be carefully discussed with a doctor.1 In children who experience side effects from anti-thyroid medications, surgery may be the preferred option.1 Radioactive iodine therapy is unlikely to be used as the long-term effects in children and teenagers are not known.1
If you are at all concerned that you or your child may be at risk of, or suffering from, thyroid problems, please discuss this with your doctor. To aid your consultation, download our Wellbeing Diary to help you keep a check of the symptoms you and / or your child are experiencing.
New mothers who have not been previously diagnosed with thyroid disease can develop problems with their thyroid within the first year after giving birth; this is called postpartum thyroiditis (PPT).1 There are several symptoms of both an underactive and overactive thyroid that new mothers can look out for.1
PPT and symptoms of an underactive thyroid
Approximately 25–45% of women who develop hypothyroid phase of PPT will experience the symptoms of an underactive thyroid.1 These include fatigue, loss of concentration, poor memory, constipation and possible depression.1
PPT and symptoms of an overactive thyroid
Between 20% and 30% of women who develop PPT experience symptoms of an overactive thyroid.1 These include fatigue, palpitations, weight loss, heat intolerance, nervousness, anxiety and irritability.1
Hyperthyroidism in PPT usually occurs in the first 6 months after the baby is born (most commonly around 3 months) and usually lasts between 1 and 2 months.1 The hypothyroidism phase of PPT usually occurs between 3 and 8 months (most commonly at 6 months) and usually last 4 to 6 months.
How is PPT treated?
PPT is generally a passing and transient condition, and treatment is not needed in all cases.
New mothers without symptoms of an underactive thyroid but with TSH changes (not more than 10miU/L) in the blood who are not planning another child do not necessarily need treatment.1
However, thyroid monitoring/checks between 4 and 8 weeks after diagnosis are recommended.1
Women with the symptoms of hypothyroidism or who are planning a subsequent pregnancy should be treated with appropriate medication.1
New mothers with symptoms of an overactive thyroid should consult their doctor for further treatment.
Follow-up for women with PPT
Even though a diagnosis of thyroid problems may be scary, PPT is not generally a long-term condition and the majority of women find their thyroid gland works normally by the end of the first year after the birth of their baby.1 Should you experience any of the symptoms outlined above, please consult your doctor.
De Groot L, Abalovich M, Alexander EK et al. Management of thyroid dysfunction during pregnancy and postpartum: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab 2012; 97: 2543–2565
Thyroid hormones interact with other, mainly reproductive, hormones.1 A normally functioning thyroid gland or adequate replacement hormones are essential for ovulation, egg implantation and maintenance of a healthy pregnancy.1
About thyroid problems and fertility
While infertility can be triggered by various factors, suboptimal function of the thyroid gland can also result in infertility, especially if thyroid disease runs in your family.1 Once the thyroid disorder is treated then you should no longer face fertility problems, providing the thyroid was the only reason for infertility.1
Know the facts
Thyroid hormones interact with other, mainly sexual, hormones.1 The right amount of thyroid hormone is necessary for normal function of the testes in men and of the ovaries in women necessary to obtain normal fertility.1 Too much (overactive thyroid) or too little (underactive thyroid) of these hormones can adversely affect male and female fertility.1 Optimal function of the thyroid gland is not only beneficial to the health of the parents — it is also crucial for the health of the baby.2 Suboptimal thyroid levels are a cause of fertility problems, increase the risk for miscarriage, premature delivery and other complications, and may impair brain development in the fetus, present in hypothyroidism too.2 Male infertility is involved in one third of couples’ inability to achieve pregnancy, while one-third of cases are related to female causes and in the remainder there are issues with both the man and woman or no cause can be identified.3
If you have been unsuccessfully trying to fall pregnant for longer than a year, ask your doctor to check your thyroid hormone status before starting other medical procedures.3 If the thyroid is the cause of your infertility, getting it under control could restore fertility and reduce your risk for health complications.1
A simple blood test, at first, can detect the amount of thyroid hormones (thyroxine and triiodothyronine) that your thyroid is secreting.4 Your doctor will be able to quickly tell you if you have hypothyroidism or hyperthyroidism.
Get your thyroid gland checked if:
You have been trying unsuccessfully to get pregnant for more than 12 months3
You have had two or more miscarriages3
You have irregular menstrual cycles3
You have any family history of infertility problems3
You have a low sperm count or a history of testicular, prostate or sexual problems3
How thyroid hormones impact male fertility
Thyroid hormones, which were previously thought not to affect male fertility, are now being recognized as having an important role in, for example, sperm production.1 The good news: correction of these disorders may restore a man’s fertility.1
The overactive thyroid
If your thyroid gland produces and releases excess thyroid hormones into the bloodstream then you have hyperthyroidism.4 Men can develop hyperthyroidism for a number of reasons, including Graves’ disease, overmedication with thyroid hormones for treatment of hypothyroidism, and the presence of thyroid nodules or an inflamed thyroid gland (known as thyroiditis).4 By speeding up your body’s metabolism, hyperthyroidism can result in many different symptoms, some of which are often mistaken for simple nervousness due to stress.4
If you are having fertility problems and also have some of the symptoms of hyperthyroidism (it is unlikely you would develop all of them) then you should bring up thyroid disease with your doctor, especially if you have a family history of thyroid disease.4
The underactive thyroid
If your thyroid gland produces insufficient thyroid hormones then you have thyroid deficiency, medically known as hypothyroidism.5 The most common causes of hypothyroidism are iodine deficiency and, where iodine deficiency is uncommon, Hashimoto’s disease, an autoimmune disease that progressively destroys your thyroid gland.5 Thyroid deficiency slows down your metabolism. Poor thyroid function is often associated with reduced libido and erectile dysfunction; furthermore, it has an adverse effect on the form and structure of sperm — all of which can give rise to infertility.1
If you are experiencing fertility problems and also have some of the symptoms of hypothyroidism then you should tell your doctor about your symptoms.
How thyroid hormones impact female fertility
Thyroid hormones interact with a woman’s reproductive hormones, estrogen and progesterone, to preserve normal function of the ovaries and maturation of the egg (oocyte).1 If your thyroid gland releases too many (hyperthyroidism) or too few (hypothyroidism) thyroid hormones then the balance of reproductive hormones can be impaired,1 with resulting thyroid-related fertility problems such as ovulation disorders, irregular periods and reduced fertility.1 Since thyroid disease is a common endocrine disorder in women of childbearing age, the first thing to do when you have trouble getting pregnant is to have your thyroid checked, especially if thyroid disease runs in your family.4
The overactive thyroid
Hyperthyroidism is 10 times more common in women than in men6 and can cause a woman to have difficulties in not only getting pregnant, but also staying pregnant.1 If your thyroid gland releases excessive amounts of thyroid hormones into the bloodstream then you are hyperthyroid.4 The most common reason for hyperthyroidism in young women is Graves’ disease, an autoimmune disorder in which antibodies mistakenly attack the thyroid gland, this stimulates the gland to overproduce thyroid hormones.4 If you experience unhealthy weight loss, this can also hamper your chances of falling pregnant.3
If hyperthyroidism is at the root of your infertility, proper treatment with a resulting optimal thyroid-stimulating hormone (TSH) level (TSH stimulates the thyroid to produce thyroid hormones) usually corrects the disturbance.1 If you are at the right TSH level but still have problems getting pregnant then you may need to consult with an endocrinologist who specializes in reproductive disorders. See also www.fertility.com.
The underactive thyroid
If you have a family history of thyroid disease or any autoimmune disease then you will be at increased risk for hypothyroidism.7 If your thyroid gland produces too few thyroid hormones, your TSH levels will increase to stimulate your thyroid gland to fill up the gap. Elevated TSH has been observed in around 5% of cases of pregnant women.8
Women who are hypothyroid may have infrequent and light menstrual bleeding, no menstrual cycles or irregular cycles due to problems with ovulation.1 The prevalence of autoimmune thyroid disease is higher in people with polycystic ovarian syndrome (PCOS),9 a condition that causes cysts on the ovaries and may lead to infertility or pregnancy complications .10
Treatment for thyroid-related infertility
If you have hypothyroidism then your thyroid gland produces insufficient thyroid hormones.7 If this is the case, you may simply have to take appropriate medication every day.7 Appropriate medication may normalize menstrual irregularities in women and sperm abnormalities and erectile dysfunction in men, and can restore fertility.1
If you have hyperthyroidism, treatment will be tailored to the specific cause and may include medication, radioactive iodine therapy or surgery.11 In women, the application of radioactive iodine treatment before pregnancy usually eliminates the need for anti-thyroid drugs. A woman should wait 4–6 months after radioactive iodine treatment before trying to become pregnant.12 Men who have had radioactive iodine treatment should wait 3–4 months before attempting to get their partner pregnant.12
Note: If you have “normal” thyroid function or your thyroid and TSH levels are regulated by treatment and you still don’t get pregnant, you should consult a fertility specialist for advice and additional treatment. See also www.fertility.com.
Bahn Chair RS, Burch HB, Cooper DS et al. Hyperthyroidism and other causes of thyrotoxicosis: management guidelines of the American Thyroid Association and American Association of Clinical Endocrinologists. Thyroid 2011; 21: 593–646
Patients with thyroid dysfunction often complain that they have mood and cognitive problems.1 An association between thyroid dysfunction and mood disorders was described by the physician C. H. Parry as early as 1825.1
Common symptoms
Some symptoms of thyroid dysfunction are similar to those seen in depression or anxiety. Symptoms that are most commonly related to hypothyroidism include forgetfulness, fatigue, mental slowness and inattention and mood swings, with depression being the predominant disorder experienced.2 Anxiety, irritability, dysphoria, mood swings and impairment in concentration are the typical psychiatric symptoms associated with hyperthyroidism.1 Loss of libido may also be associated in hyperthyroidism.3
Know the facts
About 60% of people with hyperthyroidism present with anxiety disorders, and 31–69% with depressive disorders.1 Depression frequently occurs in hypothyroidism too, where 40% of patients are said to suffer from some form of it.2
One to four percent of patients with mood disorders have hypothyroidism, and subclinical hypothyroidism occurs in 4–40% of these patients.1 This is why the American Association of Clinical Endocrinologists and the American Thyroid Association recommend that: “The diagnosis of subclinical or overt hypothyroidism must be considered in every patient with depression.”1
Treatment of mood disorders
If you have hyperthyroidism or hypothyroidism, then you are likely to develop forms of anxiety and depression.1 If your thyroid gland is underactive then you will be prone to becoming depressed.2 The good news is that, in most patients, mood disorders and cognitive issues disappear after successful treatment of their thyroid disease.2,4 If you have hypothyroidism then you will probably be given medication and it will usually take some weeks until your thyroid function returns to normal.5 If you have hyperthyroidism then you will be treated with one of the following options: anti-thyroid drugs, radioactive iodine therapy or removal of part of or the whole thyroid gland.5 Once thyroid hormone levels are in the normal range, most patients find that their anxiety and depression are resolved.2
Hage MP, Azar ST. The link between thyroid function and depression. J Thyroid Res 2012; 2012: 590648
Heinrich TW, Graham G. Hypothyroidism presenting as psychosis: myxedema madness revisited. Prim Care Companion J Clin Psychiatry 2003; 5: 260–266
Krassas GE, Poppe K, Glinoer D. Thyroid function and human reproductive health. Endocr Rev 2010; 31: 702–75
Bové KB, Watt T, Vogal A et al. Anxiety and depression are more prevalent in patients with Graves’ disease than in patients with nodular goiter. Eur Thyroid J 2014; 3: 173–178
Pregnancy causes a number of normal physiological and hormonal changes that impact the thyroid gland and may lead to increased thyroid hormone requirements.1 The baby is also dependent on the mother for its supply of thyroid hormones during pregnancy, especially in the first trimester if the fetal thyroid is not yet active.1 It is paramount that your thyroid gland is functioning properly during this critical period, and expectant mothers are advised to have the health of their thyroid checked as soon as pregnancy is detected.
Note: It is particularly important to have your thyroid checked if you suffer from endometriosis or polycystic ovary syndrome (PCOS), as you are more likely to have problems with your thyroid if you have these conditions.2
Underactive thyroid and pregnancy
If left untreated, hypothyroidism in pregnancy can be very dangerous. Thyroid hormone is critical for brain development and can leave the baby at risk for learning and development problems.1
Treatment
Treatment for hypothyroidism is the same regardless of whether a woman is pregnant or not. Taken orally, appropriate medication is recommended throughout pregnancy.1 Treatment for hypothyroidism during pregnancy is extremely important as it protects both the mother and baby from any potential future complications. Women with hypothyroidism prior to pregnancy will require a higher dose of the appropriate medication before becoming pregnant and more-frequent monitoring during pregnancy to make sure their medication dose is correct.1
Iodine deficiency and pregnancy
Iodine is vital for the production of thyroid hormones, and as your body does not produce iodine, it must be consumed as part of a healthy diet.3 Even a mild iodine shortage during pregnancy can have negative effects on the delivery and development of your baby, including your baby’s thyroid becoming underactive.1 It is therefore recommended that all pregnant and breastfeeding women take a nutritional supplement containing iodine every day.3 Women of childbearing age should have an average iodine intake of 150 micrograms per day, which should be increased to approximately 250 micrograms during pregnancy and to approximately 290 micrograms while breastfeeding.3
Overactive thyroid and pregnancy
An overactive thyroid (hyperthyroidism) in pregnant women is caused, in most cases, by Graves’ disease.1 Graves’ disease is an autoimmune disease that causes the thyroid gland to overproduce hormones, resulting in hyperthyroidism.
Failure to treat hyperthyroidism during pregnancy can increase the risk for stillbirth, premature birth and child deformities.1
The treatment for pregnant women with hyperthyroidism is sometimes different to that offered to other women, as some of the medications available can harm the unborn baby.1
Women with mild hyperthyroidism who are not experiencing symptoms will be closely monitored during their pregnancy; however, there is no call for treatment if both mother and baby are doing well.1
Women with severe hyperthyroidism who are experiencing symptoms will be treated with an anti-thyroid medication such as methimazole or propylthiouracil. The latter is usually the preferred treatment option during the first trimester of pregnancy.1
Beta-blockers can be used to help treat heart palpitations and tremor associated with hyperthyroidism but should be used sparingly during pregnancy and only until hyperthyroidism is controlled with anti-thyroid medication.2
In some cases, a pregnant woman will have surgery to partially remove the thyroid gland if she is allergic to a medication or if she requires high doses that could harm the baby.1
We use cookies to personalise content and ads, to provide social media features and to analyse our traffic. We also share information about your use of our site with our social media, advertising and analytics partners who may combine it with other information that you’ve provided to them or that they’ve collected from your use of their services. You consent to our cookies if you continue to use our website.
These cookies are necessary for the website to operate. Our website cannot function without these cookies and they can only be disabled by changing your browser preferences.
In order to continuously improve our website, we anonymously track data for statistical and analytical purposes. With these cookies we can, for example, track the number of visits or the impact of specific pages of our web presence and therefore optimize our content.
These cookies allow us to provide more comfort for you. For example, previously searched products or services can be reloaded again after revisiting our website and you won’t need to enter all the details again. We can also detect if you need assistance with using our website and therefore offer you direct customer support.
These cookies are used to display personalized content matching your interests. We can display personalized and relevant services to ensure you are always up to date on related offers.